Dr. Dilip Raja
Urologist & Andrologist
Kidney Stones
Renal Calculi, Renal stones, Urinary stones
In India, approximately 5 -7 million patients suffer from stone disease
Get in touch with us today (022) 2645 2007
Kidney stones constitute one of the commonest diseases in our country and pain due to kidney stones is known as worse than that of labour pain. In India, approximately 5 -7 million patients suffer from stone disease and at least 1/1000 of Indian population needs hospitalization due to kidney stone disease.
Geographical Distribution
- The kidney stone disease is widespread particularly in countries with dry, hot climate. These “stone belt regions” of the world are located in countries of Middle East – Dubai, Sharjah, Qatar, Muscat, Abu Dhabi, Saudi Arabia, North Africa, the Mediterranean Regions, North Western state of India and Southern State of USA and areas around the great lakes.
- In India, the “stone belt” occupies parts of Maharashtra, Gujarat, Punjab, Haryana, Delhi and Rajasthan. In these regions, the disease is so prevalent that most of the members of a family will suffer from kidney stones sometime in their lives. Removal of Kidney, Ureteric and Bladder stone procedure forms one of the commonest procedures in Urology department of the hospitals in these regions.
Causes Kidney Stones
Apparently, there are no direct causes for stone formation. However, there are few hypothesis in this regard.
- Kidney Stones: can be formed anywhere in the urinary system, like kidney, ureter, and bladder. The process by which the stone formation occurs is Supersaturation of urine.
- Hereditery :This may have some role as some people in the same family are more prone to form kidney stones.
- Diet : Diet is not a dominating factor. However, if an individual is a stone former the diet rich in calcium, oxalate & uric acid may increase the chances of stone fornation. In normal individual, diet will not play much role. More than the diet; water intake may be more responsible for kidney stone formation.
- Water Intake: If an individual is a stone former then an increased intake of water will help him pass small gravels before they become nidus for stone formation. Unfortunately, in stone belt region due to dry climate the water is hard and will, in fact, contribute to the formation of stones, if taken in large quantities.
- Medications: Medications like diureteric, excess calcium containing antacids or calcium pills will increase the chances of forming stone formation.
- Other chronic medical illness: Some chronic illness are associated with kidney stone formation specially cystic fibrosis, renal tubular acidosis and inflammatory bowel diseases etc are associated with increased risk of kidney stones formation.
Types Of Kidney Stones
There are various types of urinary stones, but the most common ones are
- Calcium oxalate.
- Uric acid.
- Struvite.
- Cystine stones.

Symptoms And Signs
- Incidental diagnosis on routine health check-ups.
- Dull aching pain in the back.
- Acute colic – This colic pain begins from the flank or the side of mid-back and comes forwards to the groin (from loin to groin). This pain is considered to be worse than labour pain, accompanied by nausea, vomiting and gaseous distension.
- Urinary tract infection.
- Increased frequency of urine.
- Pain and or burning while passing urine.
- Passage of blood in urine (Haematuria).
Investigations
- CBC, Renal Profile
- Routine urine analysis
- Crystals in urine
- Blood Cells
- Pus cells in urine
- Urine for Culture Sensitivity – To rule out UTI and select best antibiotics to treat the infection.
- X Ray KUB – To visualise the stone and any other gross pathology.
- Ultrasonography of Kidney, Ureter and Bladder (KUB) – To show the size and swelling (Hydronephrosis) of the kidney, stones in the kidney and the ureter. It does not give information about the function of the kidney.
- Intravenous Urography (IVU) – To detect the size and site of stone along with function of kidney. This is a specialized test were series of X- ray are taken after injecting the contrast media which has radiopaque property. The kidneys excrete these contrasts and kidneys are outlined on X rays and serial films are taken. This is a very useful test. It gives lot of information including size and shape of kidneys, function of kidney – comparative and individual, presence of obstructive uropathy, delineates the anatomy of kidney, ureter & bladder etc.
- CT Scan of Abdomen Pelvis /CT Urography – with or without oral or intravenous contrast. It also gives density of the renal stones in Hounsfield units ( HU). It also gives the function of the kidney. CT scan without contrast has some limitations.
Stone Work Up
In a rapid recurrent stone former – The metabolic activity for stone formation can be assessed by following investigations for the prevention of stone formation
- Serum Calcium.
- Serum Phosphorus.
- Serum Uric acid.
- 24-hour urinary calcium / 24 hrs urinary uric acid.
- Stone analysis of the retrieved calculus.
Treatment of Renal Calculi
It has been said that “once a kidney stone former, always a kidney stone former”. Once a kidney stone has been diagnosed, the choice is between expectant treatment and more aggressive forms of treatment, such as transurethral, percutaneous, or opens surgeries or extra corporeal modalities. Although some kidney stones may pass spontaneously and unless complicating conditions arise, surgical intervention may not be necessary. Thus, identification of kidney stones that are likely to pass is of utmost importance.
The primary decision is whether to apply surgical treatment or wait. Removal of kidney stones by any methodology is necessary when there is evidence of :
- Significant obstruction
- Progressive deterioration of the kidney
- Irreversible infection of the kidney (Refractory pyelonephritis)
- Unremitting pain
- Stone obstruction an infected kidney requires emergency intervention
Conservative Treatment
Most kidney stones of small size pass spontaneously in the urine without any need for intervention. The probability of a kidney stone passing down spontaneously will depend upon the size of a stone, its location, shape etc. Such patients are treated symptomatically.
Surgical Treatment Of Kidney Stones
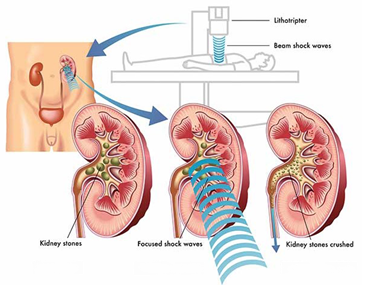
Extra Corporeal Shock Wave Lithotripsy (ESWL)
Extra Corporeal Shock Wave Lithotripsy (ESWL) is a preferred mode of treatment for kidney stones upto 1.5 cm in size. An IVU is done prior to ESWL treatment to confirm the open passage from kidney to bladder for the finer fragment to pass out after a successful ESWL treatment. ESWL machine uses highly focussed sound wave projected from outside the body to break kidney stones. The stone is generally reduced to sand like particles which subsequently passes out in the urine. More than 1.5 cm to 2 cm stones generally requires more than one or two ESWL treatments.
The primary decision is whether to apply surgical treatment or wait. Removal of kidney stones by any methodology is necessary when there is evidence of obstruction. A Double J Stent insertion becomes mandatory in most of the cases.

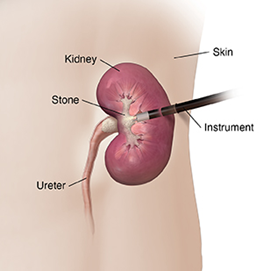
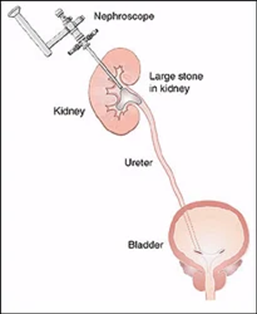
Percutaneous Nephrolithotripsy (PCNL) – Synonyms – Tunnel Surgery, Key Hole surgery for Kidney Stones
PCNL treatment is for a larger stone which are not indicated for treatment by ESWL. This procedure is generally done under general anaesthesia, spinal and /or epidural anaesthesia. In this technique the stone is removed by making a small tunnel into the kidney from the back. A fine needle is used to puncture the renal collecting system with the aid of X-ray and/or Ultrasonography, and a guide wire is led into the kidney through the needle. This tract is dilated over the guide wire and a Nephroscope (kidney telescope) is inserted into the pelvis of the kidney. The stones are visualized, fragmented using Swiss Lithoclast or laser and extracted using fine forceps, allowing the kidney to become free of stones at the end of the operation, in the vast majority patients.
This is of course an operation, needing full general anaesthesia, average 90 minutes of operation time, 3-4 day hospitalization, and an occasional need for blood transfusion. Patient returns to light work in 5-7 days’ time. Nevertheless, the operation is safe, for both the patients and the kidney. This operation has really reduced the need for open surgery (cutting surgery), which is now reserved for exceptional indications.
This Percutaneous Nephrolithotomy (PCNL) technique is used to treat kidney stones of:
- Large than 2.5 cms,
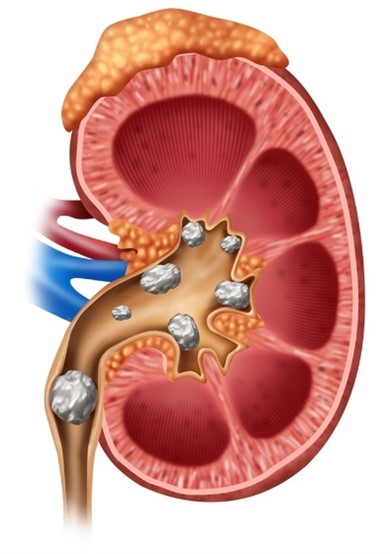
- Staghorn calculus,
- Calyceal diverticular calculus.