Now available at Breach Candy Hospital on Wednesdays 07:00 pm to 08:00 pm


Dr. Dilip Raja
Urologist & Andrologist
Case Studies
90% of Urological cases can be taken care of by Endoscopic surgery
Get in touch with us today (022) 2645 2007
Case 1
Diagnosis – A complex Case of Renal Cell Carcinoma
- Mr. M.H, 60 years of age, consulted me on October 22, 2007 with history of total painless hematuria with clots, off and on since end of July 2007.
- He did not have any other symptoms of outflow obstructions. He underwent right hernioplasty in 2004.
- He is a non diabetic and non hypertensive and does not suffer from any cardio respiratory disorders.
- Physical Examination was essentially normal. Rectal Examination revealed Benign Hypertrophy (BPH) of prostate Grade I approximately 10 – 15 gms. Routine Biochemical Parameters were within normal limits. His urine analysis showed microscopic hematuria. X-Ray chest normal. His PSA was 1 ng/dl. His uroflowmetry was normal. His Ultrasonography revealed bilateral tiny renal calculi with no evidence of hydronephrosis.
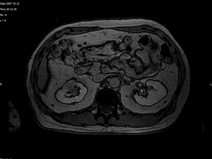
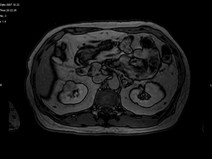
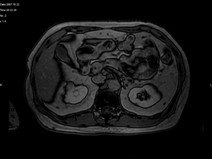
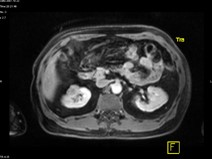
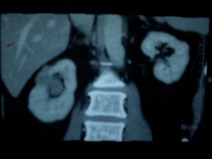
- His repeat ultrasonography revealed 4.4 x 3.5 x 3.4 cm sized ill defined hypoechoic lesion in the mid region of right kidney arising from the renal parenchyma. The lesion caused contour irregularity and indenting of the echogenic fat of the sinus. Left kidney was normal.
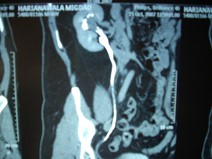
- His ultra fast MDCT urography revealed a soft tissue mass in the calyces of upper moiety of the right kidney. The renal function was normal bilaterally. The CT scan concluded as possibility of transitional cell carcinoma.
- Impression –A parenchymal mass in the anterior aspect of upper pole of right kidney with an exophytic component and invasion in upper pole calyx most likely a renal cell carcinoma.
- Subsequently, Mr. M. H underwent Right Radical Nephrectomy on October 25, 2007 through 11th rib bed incision by flank approach. The renal artery and the vein were approached first retroperitoneally and were divided between the ligatures. The kidney with its Genota’s Fascia and the supra renal glands was mobilized and removed after dividing the ureter as low as possible up to the pelvic brim.
- The frozen section of the kidney and the specimen revealed papillary neoplasm favourable with features of papillary renal carcinoma. No features of classical Transitional Cell Carcinoma were seen. Parenchymal Tumour reached up to renal pelvis and polypoid projections protruded loosely into it.
- Mr. M. H recovered from the procedure uneventfully and was discharged from the hospital on 3rd post operative day with the advice to come back for the removal of the sutures on the 10th post operative day.
- Mr. M.H was followed up and has been doing well. Histopathology of the specimen revealed Right Kidney – Papillary cell carcinoma Type 1 Fuhrman Nuclear Grade II confined by Gerota’s fascia (stage 2 – Robson System, TNM – T3a). Hilar nodes – No metastasis. Hilar blood vessels – No tumor involvement. Ureter – No tumor involvement. Adrenal – No tumor involvement.





Case 2
Diagnosis – A Universal Case of Right Lower 3rd Ureteric Calculus with Hydronephrosis and ‘Urinoma’
- Mrs. A.B., 73 years of age consulted me with history of total painless hematuria 15 days back. This was accompanied by pain in the left lumbar region. The episode lasted for 2 days. She also suffers from diabetes mellitus and hypertension for last 10 years. She underwent Coronary Angiography for Ischemic heart disease and has been on medication since then. She underwent Cystoscopy and biopsy of bladder tumour outside which revealed low grade transitional cell Carcinoma.
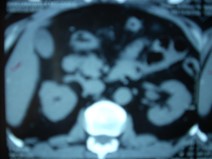
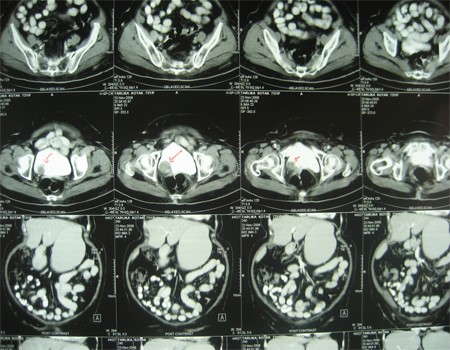
- Physical Examination was essentially normal. The CT scan revealed a lobulated hypodense 3.8 X 3.5 cms sized mildly enhancing soft tissue mass lesion in the right postero-lateral aspect of Urinary Bladder. This is involving the right vesico- ureteric junction. A streaking of peri vesical fat is noted. The urinary bladder otherwise shows normal distension and wall thickness.
- She was advised to undergo Cystoscopy and Trans Urethral Resection of Bladder Tumor (TURBT) for which she was admitted to the hospital. She underwent Trans Urethral Resection of Bladder Tumor (TURBT). At Cystoscopy she had a papillary tumor arising just beyond the right ureteric. The right ureteric orifice could not be seen. Right ureteric orifice however, was successfully catheterized using number 5 ureteric catheter. There was no intra luminal lesion in the right ureteric orifice and the papillary growth of the bladder was resected saving the right ureteric orifice. The mass was completely resected and the histopathology revealed Papillary Urothelial Carcinoma (Grade III) of the Urinary Bladder.
- Mrs. A.B. was discharged from the hospital in satisfactory condition. Post operative day she passed urine satisfactorily. She has been advised for a follow up after 10 days with urine analysis and she is doing well. She is also advised to come back for check Cystoscopy after 3 months. Mrs. A.B is now fit to resume her normal activities.
Case 3
Diagnosis – A Case of Transitional Cell Carcinoma of the Bladder
- Mrs. A.B., 73 years of age consulted me with history of total painless hematuria 15 days back. This was accompanied by pain in the left lumbar region. The episode lasted for 2 days. She also suffers from diabetes mellitus and hypertension for last 10 years. She underwent Coronary Angiography for Ischemic heart disease and has been on medication since then. She underwent Cystoscopy and biopsy of bladder tumour outside which revealed low grade transitional cell Carcinoma.
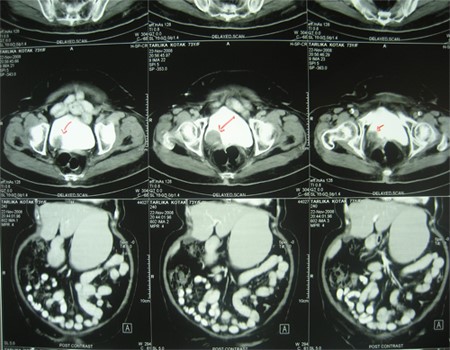
- Physical Examination was essentially normal. The CT scan revealed a lobulated hypodense 3.8 X 3.5 cms sized mildly enhancing soft tissue mass lesion in the right postero-lateral aspect of Urinary Bladder. This is involving the right vesico- ureteric junction. A streaking of peri vesical fat is noted. The urinary bladder otherwise shows normal distension and wall thickness.
- She was advised to undergo Cystoscopy and Trans Urethral Resection of Bladder Tumor (TURBT) for which she was admitted to the hospital. She underwent Trans Urethral Resection of Bladder Tumor (TURBT). At Cystoscopy she had a papillary tumor arising just beyond the right ureteric. The right ureteric orifice could not be seen. Right ureteric orifice however, was successfully catheterized using number 5 ureteric catheter. There was no intra luminal lesion in the right ureteric orifice and the papillary growth of the bladder was resected saving the right ureteric orifice. The mass was completely resected and the histopathology revealed Papillary Urothelial Carcinoma (Grade III) of the Urinary Bladder.
- Mrs. A.B. was discharged from the hospital in satisfactory condition. Post operative day she passed urine satisfactorily. She has been advised for a follow up after 10 days with urine analysis and she is doing well. She is also advised to come back for check Cystoscopy after 3 months. Mrs. A.B is now fit to resume her normal activities.




Case 4
Diagnosis – A Case of An unusual Primitive Neuroectodermal Tumour of the Kidney
- Mr. B.R, 28 years of age consulted me with history of pain in right lumbar region for last 4 – 5 weeks. This was associated with gross total painless intermittent hematuria without clots once in 2 – 3 weeks. He also complained of fever about 2 months back and his hematuria has been persisting for the last 2 days. He does not suffer from any other medical or surgical illness.
- Physical Examination was essentially normal except for the large ballotable mass was felt in the right hypochondrium and right lumbar region. This was not tender. Routine Biochemical Parameters were within normal limits. His urine revealed significant microscopic hematuria with urinary tract infection.
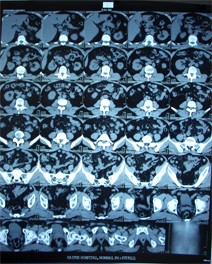
- His ultrasonography revealed a hypoechoic mass in the lower pole of the right kidney. CT scan of the abdomen and pelvis revealed a large mass lesion involving the right kidney with non-visualization of the right ureter. The lesion abuts the duodenum, head of pancreas, psoas muscles and ascending colon with stranding of the adjacent fat planes. Neoplastic etiology is likely? RCC. Centimetre sized retroperitoneal nodes are noted. X-ray chest was normal.
- Subsequently Mr. B.R was admitted to hospital. He was subjected to Laparoscopic Right Radical Nephrectomy under general anaesthesia. Multiple ports were used and right colon was mobilized medially. Duodenum was kocherised. The hilum was approached and the renal artery was dissected free. It was cut between the ligatures. Renal vein was stapled. The ureter was mobilized and was clipped. The gonadal veins were also clipped. The specimen was freed and was removed through an extended transverse Pfannenstiel like incision and the kidney was removed and sent for histopathology examination.
- The histopathology revealed: The Right Kidney – Malignant, Poorly Differentiated Round Cell Tumour – Primitive Neuroectodermal Tumor (PNET). Tumour invades Ureter. Tumour invades Adrenal (not separately identified from tumour) Peri renal fat invaded. Gerota’s Fascia not involved. Renal Hilac vessels – not involved. Mr. B.R. recovered from the procedure well and was discharged from the hospital.
- Further, the histopathology slides were sent for another opinion which revealed Primitive Neuroectodermal Tumor of the Kidney. The tumour cells express Mic2. They are negative for CK & vimentin.
- Post operatively he was also subjected to whole body PET CT scan which shows minimally active left para-aortic nodes. Uptake in the left adrenal? significance.
- Mr. B.R has further been referred to a medical Oncologist for further directions. In the meanwhile, skin staples were removed and wound was healthy. Medical Oncologist has advised him to take chemotherapy for Primitive Neuroectodermal Tumor with ICE x 6 such. He is pursuing the treatment with medical oncologist. Mr. B.R. is now doing well and is fit to resume his normal activities.